Human African trypanosomiasis (HAT), also known as sleeping sickness, is a parasitic disease that attacks the central nervous system, causing severe neurological disorders and death if left untreated. It is transmitted by the bite of the ‘Glossina’ insect, commonly known as the tsetse fly.
The disease mostly affects poor populations in rural areas where agriculture, fishing, animal husbandry, or hunting are the main source of livelihood. Typically, HAT is not found in urban areas, although cases have been reported in suburban areas of big cities in 36 sub-Saharan African countries where the disease is endemic. Travelers also risk becoming infected if they go to regions where the insect is common.
HAT wreaked havoc in Africa at different times in the 20th century but over the past twenty years, huge efforts made by a broad coalition of stakeholders, curbed the last epidemic.

Human African trypanosomiasis takes two forms, depending on the parasite involved: Trypanosoma brucei gambiense, found in 24 countries in west and central Africa, accounts for 98% of reported cases of sleeping sickness and causes a chronic infection.
A person can be infected for months or even years without major signs or symptoms of the disease. When more evident symptoms emerge, the patient is often already in an advanced disease stage.
Trypanosoma brucei rhodesiense is found in 13 countries in eastern and southern Africa. This form represents under 2% of reported cases and causes an acute infection that invades the central nervous system.
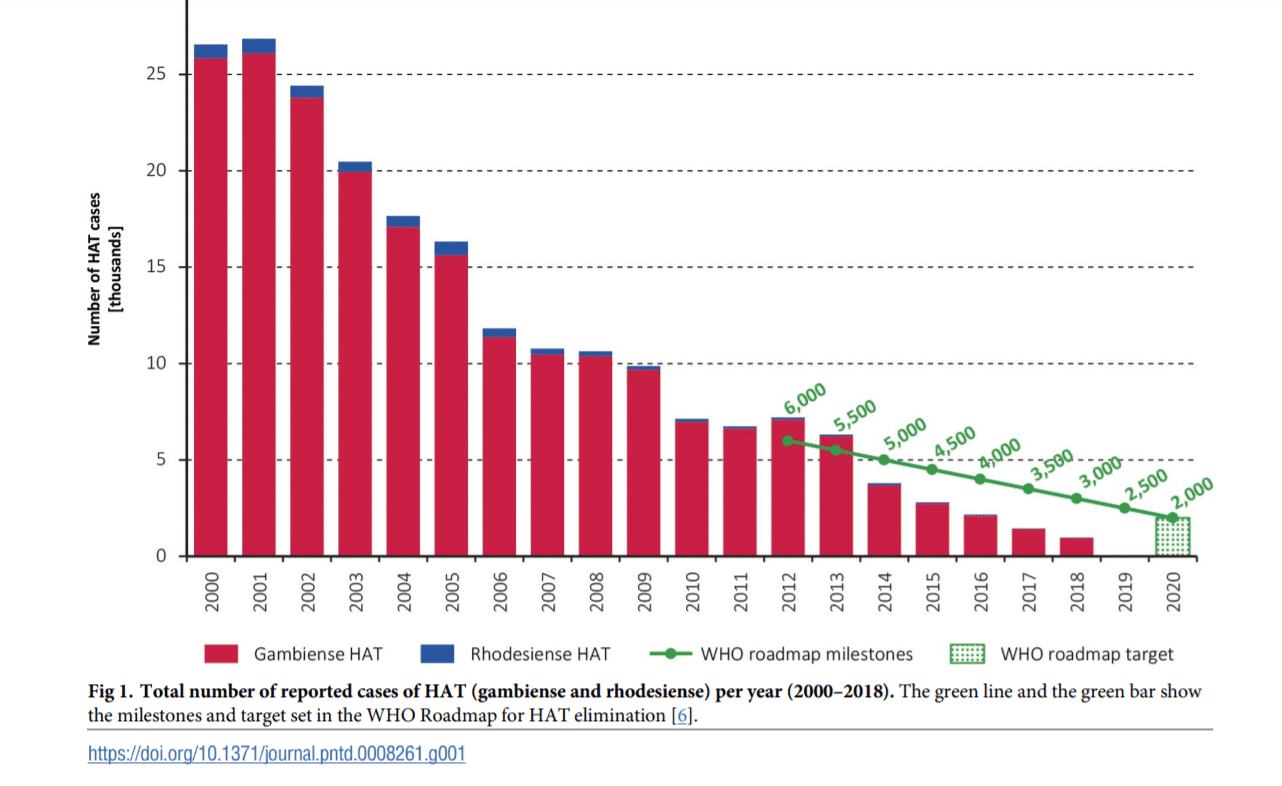
A detailed analysis of data systematically collected by WHO in the years 2000-2018 in the HAT Atlas was published in PLoS NTDs showing the updated picture of the elimination trends in this disease. The analysis of global indicators and milestones of the WHO NTD roadmap has been updated to 2018 and recently published. The disease occurrence, the geographical distribution and the control activities show that:
- 977 cases of HAT were reported in 2018, down from 2,164 in 2016.
- The area at moderate or high risk of HAT has shrunk to less than 200,000 square kilometres. More than half of this area is in the Democratic Republic of the Congo. In the last 10 years, over 70% of reported cases occurred in the Democratic Republic of the Congo.
- Health facilities providing diagnosis and treatment for HAT have increased since the last survey, meanwhile active screening is maintained at similar levels.
The number of cases, the main global indicator, is already well within the 2020 target (i.e. 2,000 cases). The areas at moderate or higher risk (i.e. > 1 case/10,000 people/year) are also nearing the 2020 target. The reliability of these data is backed by a reinforced coverage of the populations at risk by surveillance and control activities, providing strong evidence that global elimination of the disease is advancing.
There is no vaccine or drug for prophylaxis and preventive measures are aimed at minimizing contact with tsetse flies. Sleeping sickness is curable with medication but is fatal if left untreated. Surveillance networks, such as ProMED-mail and TropNetEurop should be maintained and expanded to ensure access to institutional databases. Due to the success of surveillance systems in Western countries, the possibility of introducing similar ‘alarm’ systems for HAT in Africa should be explored. Innovation in HAT control and surveillance is still needed but the 2030 goal of elimination as interruption of HAT transmission is on track.


